Apr
26
2024
 Most people have watched large flocks of birds. They are fascinating, and have interested scientists for a long time. How, exactly, do so many birds maintain their cohesion as a flock? It’s obviously a dynamic process, but what are the mechanisms?
Most people have watched large flocks of birds. They are fascinating, and have interested scientists for a long time. How, exactly, do so many birds maintain their cohesion as a flock? It’s obviously a dynamic process, but what are the mechanisms?
When I was young I was taught that each flock had a leader, and the other birds were ultimately just following that leader. When two smaller flocks combined into a larger flock, then one of those leaders become dominant and takes over the combined flock. But this explanation is largely untrue. It actually depends a great deal on the species of bird and the type of flock.
The “follow the leader” method is essentially what is happening with the V formations. These are obviously very different from the murmurations of small birds morphing like a giant flying amoeba. Some species, like pigeons, use a combined strategy, still following a leader, but more of a hierarchy of leaders, which can change over time.
For the more dynamic flocks, like starlings, researchers found that there is no leader or hierarchy. Every bird is just following the flock itself. It is a great example of an emergent phenomenon in nature. It’s like ants working in a colony or a bee hive – each individual bee or ant does not really know what the entire colony is doing, and there is no leader or foreman calling the shots or directing traffic. Each individual is just following a simple algorithm, and the collective complexity emerges from that.
Continue Reading »
Apr
23
2024
 The most recent episode of John Oliver, Last Week Tonight, featured a discussion of the UFO phenomenon. I’m always interested, and often disappointed, in how the mainstream media portrays skeptical topics. One interesting addition here is that Oliver actually referenced an SGU episode, the one in which we interviewed Jimmy Carter about his UFO sighting. Unfortunately the rest of the episode was a bit of a let down.
The most recent episode of John Oliver, Last Week Tonight, featured a discussion of the UFO phenomenon. I’m always interested, and often disappointed, in how the mainstream media portrays skeptical topics. One interesting addition here is that Oliver actually referenced an SGU episode, the one in which we interviewed Jimmy Carter about his UFO sighting. Unfortunately the rest of the episode was a bit of a let down.
Oliver is the first to acknowledge that he is not a journalist. He’s a comedian. But comedians often give biting satire of our culture and society, and Oliver has developed a specific niche. He essentially picks a topic and makes the point that – we’re doing it wrong, we can do better. Oliver also has a staff of researchers, so he is not jut making stuff up or giving superficial observations. In general I find he does an excellent job, giving a descent overview of a topic and making important observations. But of course many of the topics he covers are too complex to do justice in a 20 minute comedy routine, but he usually manages to hit the important points.
His piece of UFOs was very typical of his general approach. All storytellers (whether you are a journalist, blog writer, or comedian) have a narrative, some organizing point or argument that you are making. Otherwise a piece is just a list of facts or assertions. Oliver’s series has a narrative (as I said, we’re doing it wrong), and each episode has a narrative within that framework. For the UFO piece his main narrative was that the US government is doing UFO research wrong, and this is being driven by the underlying fact that most people interested in UFOs fall into one of two groups, true believers or hardline skeptics. True believers will believe anything, no matter how ridiculous, and hardline skeptics just roll their eyes dismissively, chilling genuine research.
Continue Reading »
Apr
22
2024
I recently received the following question to the SGU e-mail:
“I have had several conversations with friends/colleagues lately regarding indigenous beliefs/stories. They assert that not believing these based on oral histories alone is morally wrong and ignoring a different cultures method of knowledge sharing. I do not want to be insensitive, and I would never argue this point directly with an indigenous person (my friends asserting these points are all white). But it really rubs me the wrong way to be told to believe things without what I would consider more concrete evidence. I’m really not sure how to comport myself in these situations. I would love to hear any thoughts you have on this topic, as I don’t have many skeptical friends.”
I also frequently encounter this tension, between a philosophical dedication to scientific methods and respect of indigenous cultures. Similar tensions come up in other contexts, such as indigenous cultures that hunt endangered species. These tensions are sometimes framed as “decolonization” defined as “the process of freeing an institution, sphere of activity, etc. from the cultural or social effects of colonization.” Here is a more detailed description:
“Decolonization is about “cultural, psychological, and economic freedom” for Indigenous people with the goal of achieving Indigenous sovereignty — the right and ability of Indigenous people to practice self-determination over their land, cultures, and political and economic systems.”
I completely understand this concept and think the project is legitimate. To “decolonize” an indigenous culture you have to do more than just physically remove foreign settlers. Psychological and cultural colonization is harder to remove. And often cultural colonization was very deliberate, such as missionaries spreading the “correct” religion to “primitive” people.
Continue Reading »
Apr
19
2024
 Boston Dynamics (now owned by Hyundai) has revealed its electric version of its Atlas robot. These robot videos always look impressive, but at the very least we know that we are seeing the best take. We don’t know how many times the robot failed to get the one great video. There are also concerns about companies presenting what the full working prototype might look like, rather than what it actually currently does. The state of CGI is such that it’s possible to fake robot videos that are indistinguishable to the viewer from real ones.
Boston Dynamics (now owned by Hyundai) has revealed its electric version of its Atlas robot. These robot videos always look impressive, but at the very least we know that we are seeing the best take. We don’t know how many times the robot failed to get the one great video. There are also concerns about companies presenting what the full working prototype might look like, rather than what it actually currently does. The state of CGI is such that it’s possible to fake robot videos that are indistinguishable to the viewer from real ones.
So it’s understandable that these robot reveal videos are always looked at with a bit of skepticism. But it does seem that pushback does have an effect, and there is pressure on robotics companies to be more transparent. The video of the new Atlas robot does seem to be real, at least. Also, these are products for the real world. At some point the latest version of Atlas will be operating on factory floors, and if it didn’t work Boston Dynamics would not be sustainable as a company.
What we are now seeing, not just with Atlas but also Tesla’s Optimus Gen 2, and others, is conversion to all electric robots. This makes them smaller, lighter, and quieter than the previous hydraulic versions. They are also not tethered to cables as previous versions.
My first question was – what is the battery life? Boston Dynamics says they are “targeting” a four hour battery life for the commercial version of the Atlas. I love that corporate speak. I could not find a more direct answer in the time I had to research this piece. But four hours seems reasonable – the prior version from 2015 had about a 90 minute battery life depending on use. Apparently the new Atlas can swap out its own battery.
Continue Reading »
Apr
16
2024
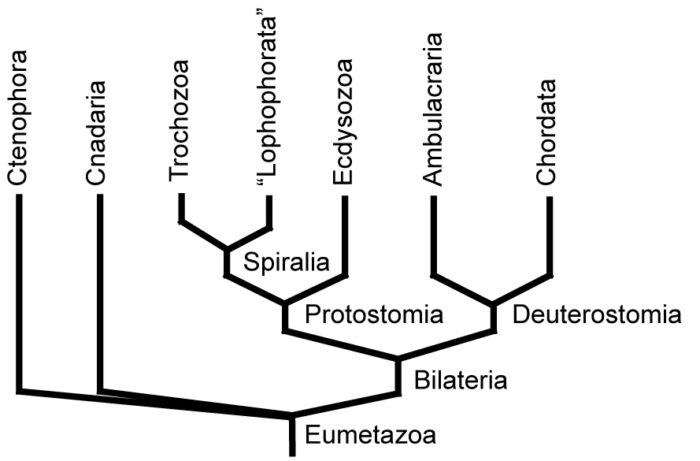 Evolution deniers (I know there is a spectrum, but generally speaking) are terrible scientists and logicians. The obvious reason is because they are committing the primary mortal sin of pseudoscience – working backwards from a desired conclusion rather than following evidence and logic wherever it leads. They therefore clasp onto arguments that are fatally flawed because they feel they can use them to support their position. One could literally write a book using bad creationist arguments to demonstrate every type of poor reasoning and pseudoscience (I should know).
Evolution deniers (I know there is a spectrum, but generally speaking) are terrible scientists and logicians. The obvious reason is because they are committing the primary mortal sin of pseudoscience – working backwards from a desired conclusion rather than following evidence and logic wherever it leads. They therefore clasp onto arguments that are fatally flawed because they feel they can use them to support their position. One could literally write a book using bad creationist arguments to demonstrate every type of poor reasoning and pseudoscience (I should know).
A classic example is an argument mainly promoted as part of so-called “intelligent design”, which is just evolution denial desperately seeking academic respectability (and failing). The argument goes that natural selection cannot increase information, only reduce it. It does not explain the origin of complex information. For example:
A big obstacle for evolutionary belief is this: What mechanism could possibly have added all the extra information required to transform a one-celled creature progressively into pelicans, palm trees, and people? Natural selection alone can’t do it—selection involves getting rid of information. A group of creatures might become more adapted to the cold, for example, by the elimination of those which don’t carry the genetic information to make thick fur. But that doesn’t explain the origin of the information to make thick fur.
I am an educator, so I can forgive asking a naive question. Asking it in a public forum in order to defend a specific position is more dodgy, but if it were done in good faith, that could still propel public understanding forward. But evolution deniers continue to ask the same questions over and over, even after they have been definitively answered by countless experts. That demonstrates bad faith. They know the answer. They cannot respond to the answer. So they pretend it doesn’t exist, or when confronted directly, respond with the equivalent of, “Hey, look over there.”
Continue Reading »
Apr
15
2024
 Generative AI applications seem to be on the steep part of the development curve – not only is the technology getting better, but people are finding more and more uses for it. It’s a new powerful tool with broad applicability, and so there are countless startups and researchers exploring its potential. The last time, I think, a new technology had this type of explosion was the smartphone and the rapid introduction of millions of apps.
Generative AI applications seem to be on the steep part of the development curve – not only is the technology getting better, but people are finding more and more uses for it. It’s a new powerful tool with broad applicability, and so there are countless startups and researchers exploring its potential. The last time, I think, a new technology had this type of explosion was the smartphone and the rapid introduction of millions of apps.
Generative AI applications have been created to generate text, pictures, video, songs, and imitate specific voices. I have been using most of these apps extensively, and they are continually improving. Now we can add another application to the list – generating virtual environments. This is not a public use app, but was developed by engineers for a specific purpose – to train robots.
The application is called holodeck, after the Star Trek holodeck. You can use natural language to direct the application to build a specific type of virtual 3D space, such as “build me a three bedroom single floor apartment” or “build me a music studio”. The application uses generative AI technology to then build the space, with walls, floor, and ceiling, and then pull from a database of objects to fill the space with appropriate things. It also has a set of rules for where things go, so it doesn’t put a couch on the ceiling.
The purpose of the app is to be able to generate lots of realistic and complex environments in which to train robot navigation AI. Such robotic AIs need to be trained on virtual spaces so they can learn how to navigate out there is the real world. Like any AI training, the more data the better. This means the trainers need millions of virtual environments, and they just don’t exist. In an initial test, Holodeck was compared to an earlier application called ProcTHOR and performed significantly better. For example, when asked to find a piano in a music studio a ProcTHOR trained robot succeeded 6% of the time while a Holodeck trained robot succeeded 30% of the time.
Continue Reading »
Apr
11
2024
 Over the weekend when I was in Dallas for the eclipse, I ran into a local businessman who works in the energy sector, mainly involved in new solar projects. This is not surprising as Texas is second only to California in solar installation. I asked him if he is experiencing a backlog in connections to the grid and his reaction was immediate – a huge backlog. This aligns with official reports – there is a huge backlog and its growing.
Over the weekend when I was in Dallas for the eclipse, I ran into a local businessman who works in the energy sector, mainly involved in new solar projects. This is not surprising as Texas is second only to California in solar installation. I asked him if he is experiencing a backlog in connections to the grid and his reaction was immediate – a huge backlog. This aligns with official reports – there is a huge backlog and its growing.
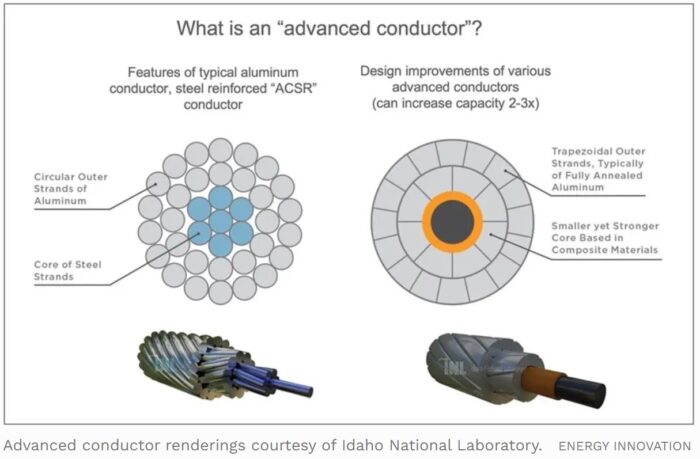
In fact, the various electrical grids may be the primary limiting factor in transitioning to greener energy sources. As I wrote recently, energy demand is increasing, faster than previously projected. Our grid infrastructure is aging, and mainly uses 100 year old technology. There are also a number of regulatory hurdles to expanding and upgrading the grid. There is good news in this story, however. We have at our disposal the technology to virtually double the capacity of our existing grid, while reducing the risk of sparking fires and weather-induced power outages. This can be done cheaper and faster than building new power lines.
The process is called reconductoring, which just means replacing existing power lines with more advanced power lines. I have to say, I falsely assumed that all this talk about upgrading the electrical grid included replacing existing power lines and other infrastructure with more advanced technology, but it really doesn’t. It is mainly about building new grid extensions to accommodate new energy sources and demand. Every resource I have read, including this Forbes article, give the same primary reason why this is the case. Utility companies make more money from expensive expansion projects, for which they can charge their customers. Cheaper reconductoring projects make them less money.
Continue Reading »
Apr
08
2024
 I am currently in Dallas Texas waiting to see, hopefully, the 2024 total solar eclipse. This would be my first total eclipse, and everything I have heard indicates that it is an incredible experience. Unfortunately, the weather calls for some clouds, although forecasts have been getting a little better over the past few days, with the clouds being delayed. Hopefully there will be a break in the clouds during totality.
I am currently in Dallas Texas waiting to see, hopefully, the 2024 total solar eclipse. This would be my first total eclipse, and everything I have heard indicates that it is an incredible experience. Unfortunately, the weather calls for some clouds, although forecasts have been getting a little better over the past few days, with the clouds being delayed. Hopefully there will be a break in the clouds during totality.
Actually there is another reason to hope for a good viewing. During totality the temperature will drop rapidly. This can cause changes in pressure that will temporarily disperse some types of clouds.
I am prepared with eclipse glasses, a pair of solar binoculars, and one of my viewing companions has a solar telescope. These are all certified and safe, and I have already used the glasses and binoculars extensively. You can use them to view the sun even when there is not an eclipse. With the binoculars you can see sunspots – it’s pretty amazing.
Continue Reading »
Apr
02
2024
 On a recent SGU live streaming discussion someone in the chat asked – aren’t frivolous AI applications just toys without any useful output? The question was meant to downplay recent advances in generative AI. I pointed out that the question is a bit circular – aren’t frivolous applications frivolous? But what about the non-frivolous applications?
On a recent SGU live streaming discussion someone in the chat asked – aren’t frivolous AI applications just toys without any useful output? The question was meant to downplay recent advances in generative AI. I pointed out that the question is a bit circular – aren’t frivolous applications frivolous? But what about the non-frivolous applications?
Recent generative AI applications are a powerful tool. They leverage the power and scale of current data centers with the massive training data provided by the internet, using large language model AI tools that are able to find patterns and generate new (although highly derivative) content. Most people are likely familiar with this tech through applications like ChatGPT, which uses this AI process to generate natural-language responses to open ended “prompts”. The result is a really good chat bot, but also a useful interface for searching the web for information.
This same technology can generate output other than text. It can generate images, video, and music. The results are technically impressive (if far from perfect), but in my experience not genuinely creative. I think these are the fun applications the questioner was referring to.
But there are many serious applications of this technology in development as well. An app like ChatGPT can make an excellent expert system, searching through tons of data to produce useful information. This can have many practical applications, from generating lists of potential diagnoses for doctors to consider, to writing first-draft legal contracts. There are still kinks to be worked out, but the potential is clearly amazing.
Continue Reading »
Apr
01
2024
I have not written before about Havana Syndrome, mostly because I have not been able to come to any strong conclusions about it. In 2016 there was a cluster of strange neurological symptoms among people working at the US Embassy in Havana, Cuba. They would suddenly experience headaches, ringing in the ears, vertigo, blurry vision, nausea, and cognitive symptoms. Some reported loud whistles, buzzing or grinding noise, usually at night while they were in bed. Perhaps most significantly, some people who reported these symptoms claim that there was a specific location sensitivity – the symptoms would stop if they left the room they were in and resume if they returned to that room.
These reports lead to what is popularly called “Havana Syndrome”, and the US government calls “anomalous health incidents” (AHIs). Eventually diplomats in other countries also reported similar AHIs. Havana Syndrome, however, remains a mystery. In trying to understand the phenomenon I see two reasonable narratives or hypotheses that can be invoked to make sense of all the data we have. I don’t think we have enough information to definitely reject either narrative, and each has its advocates.
One narrative is that Havana Syndrome is caused by a weapon, thought to be a directed pulsed electromagnetic or acoustic device, used by our adversaries to disrupt American and Canadian diplomats and military personnel. The other is that Havana Syndrome is nothing more than preexisting conditions or subjective symptoms caused by stress or perhaps environmental factors. All it would take is a cluster of diplomats with new onset migraines, for example, to create the belief in Havana Syndrome, which then takes on a life of its own.
Both hypotheses are at least plausible. Neither can be rejected based on basic science as impossible, and I would be cautious about rejecting either based on our preexisting biases or which narrative feels more satisfying. For a skeptic, the notion that this is all some kind of mass delusion is a very compelling explanation, and it may be true. If this turns out to be the case it would definitely be satisfying, and we can add Havana Syndrome to the list of historical mass delusions and those of us who lecture on skeptical topics can all add a slide to our Powerpoint presentations detailing this incident.
Continue Reading »





